

The M23 insurgency has absorbed the attention of the Democratic Republic of the Congo’s government and led to a flurry of regional peace efforts over the past year. Yet the conflict is just one of many driving humanitarian needs in the country.
Of the more than 100 armed groups active in DRC’s eastern provinces, one of the oldest and most violent is the Allied Democratic Forces (ADF), a militant movement of Ugandan origins that has pledged allegiance to the so-called Islamic State (IS).
With the spotlight on the M23 – which is backed by Rwanda and has seized large chunks of territory in the east – The New Humanitarian spent time speaking with survivors of ADF atrocities and health workers addressing the conflict’s fallout.
“I have been supporting displaced people of different wars for 20 years… [but] the ADF massacres have become serious and we have never experienced such killings,” said Marie-Jeanne Masika, who works for a local NGO helping conflict victims.
Interviewees said recent measures taken to combat the ADF – from a joint Uganda-DRC military intervention to the introduction of martial law – have failed to improve security for civilians.
Instead, the militants have expanded geographically, carrying out massacres, abductions, and bombings in urban areas that have struck targets including a government building, a cinema, and a church in recent months.
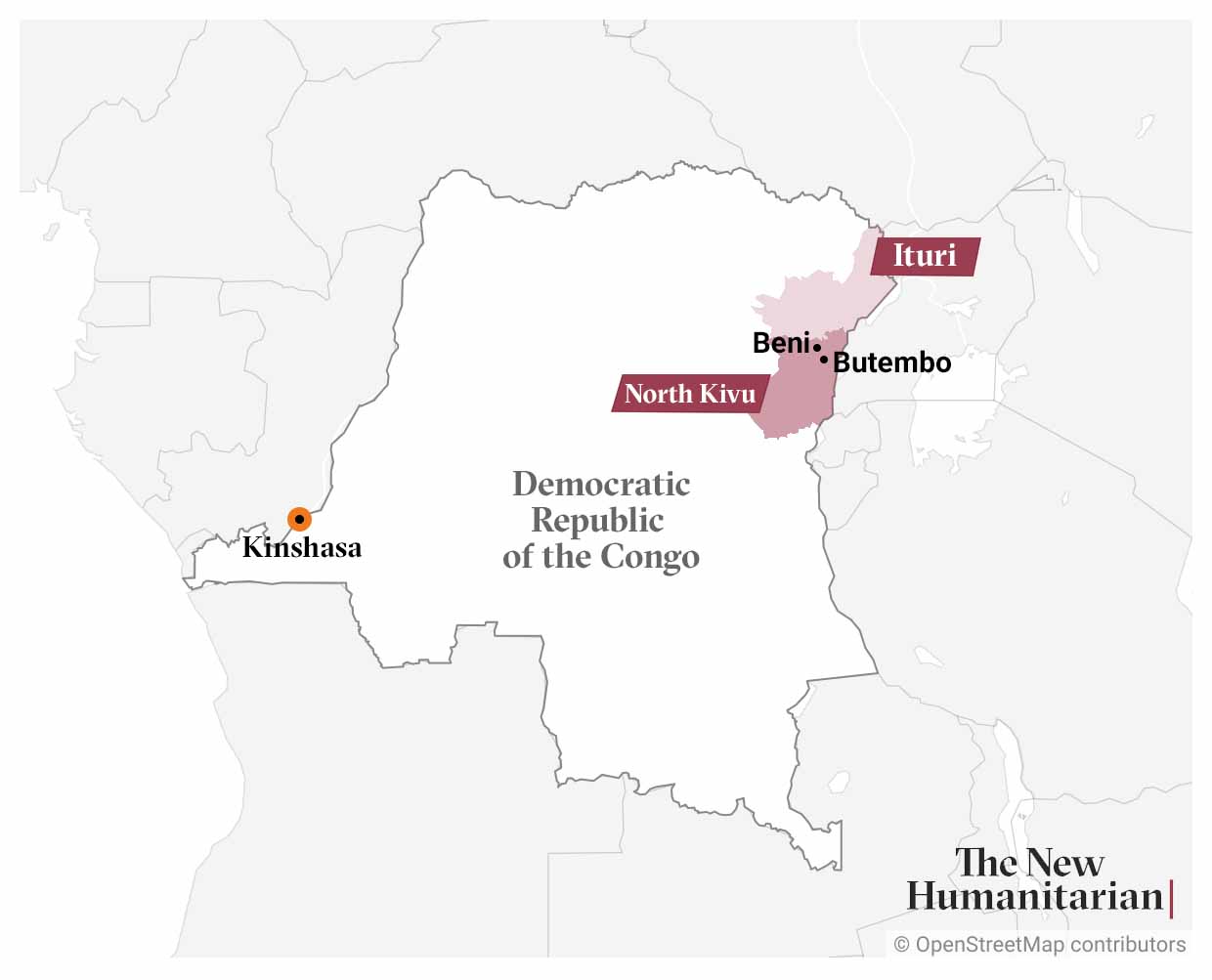
Those affected by the long-running violence – which centres on North Kivu and Ituri provinces – raised warnings of a rising mental health toll. Yet local health workers said there is an absence of support for those needing psychosocial services.
“Today, we must no longer reduce humanitarian assistance to the sole distribution of provisions… to victims,” said Masika. “A big problem also remains psychosocial care to avoid having mental illnesses in the future.”
‘We are in so much pain’
The ADF formed in 1995 after members fled to DRC amid military pressure in Uganda. It has its roots in the repression of Ugandan Muslims, though its complex history and modus operandi is obscured by narratives that focus solely on its Islamist orientation.
Military operations, including by UN peacekeepers, are frequently launched against the group. Yet they often result in ADF reprisal attacks, which are designed to punish civilians who support the army and pressure the government to end offensives.
Recent ADF raids have sought to undermine support for Uganda’s operations. That mission – which may be guided by economic interests rather than security concerns – was launched after IS claimed a triple suicide bombing in Kampala in late 2021.
How are the ADF and IS linked?
Recent reports on the ADF have focused on its ties to IS. Communication between the two movements appears to have strengthened in recent months, and the ADF may be adopting some of the habits and practices of the global group.
UN experts said in a report last year that the ADF is considered an option for recruits wanting to join IS. However, the experts said they have not found evidence of IS command and control over the ADF, nor signs of direct financial support.
Researchers that have studied the ADF are often wary of overplaying the IS connection. Instead, they emphasise the ADF’s complex history, the varying motivations of its fighters, and the way it has become enmeshed in local politics, conflicts, and business.
Researchers also point out that the Congolese army has at different stages been accused of inaction or direct complicity in ADF violence, compromising the effectiveness of military campaigns.
Earlier this month, The New Humanitarian attended a meeting of displaced people who had fled recent ADF massacres. Held at a cathedral in Butembo, a town in North Kivu, the convening highlighted the suffering caused by the conflict.
Kavugho Sikiliza, 42, said she had lost four of her relatives, including her son and daughter-in-law, in an ADF attack in Bashu chiefdom – in the North Kivu territory of Beni – last September.
“We suffer so much. We have abandoned our fields and we no longer find anything to eat,” Kavugho said. “Today, we are spending the night in the bush; we have orphans who are struggling to [eat].”
Next to Kavugho sat Yoha Nyasavo Bibiche. Six months ago, she saw her son killed by ADF rebels in Mungamba, in Ituri province. She is now living in Butembo but was recently forced out of her house there because she couldn't afford rent.
“As we were about to harvest, the ADF attacked the village and stabbed my son, who is dead,” said Bibiche. “We no longer have a home. Eating, dressing – it has become a headache.”
Mental health toll
The cumulative impact of attacks – which have killed thousands over the past decade – have led to serious mental health challenges, according to survivors and medical staff from three psychiatric centres The New Humanitarian visited in Beni and Butembo.
Esdras Pika, a psychologist at a health centre in Butembo, said his clinic treats survivors of ADF killings, kidnap victims, and farmers and traders struggling to cope with the loss of their livelihoods.
“Before 2015, the reasons that led patients to be admitted to mental healthcare here were often drug abuse [and] cases of romantic disappointment,” Pika said. “But today, most of the patients who come to us are victims of insecurity.”
Kakule Kisonia, from Beni territory, said his brother went to the local Muyisa psychiatric centre after witnessing a recent ADF attack that cost the lives of his wife, sister, and two of his children. Kisonia said his brother’s behaviour changed after the attack.
“Every night he shouted: Ba Nalu! Ba Nalu! [a reference to the ADF in Swahili],” Kisonia said. “Each time a neighbour came, he shouted that it was the ADF, and did not hesitate to take either a wooden stick or a machete to attack the visitors.”
More support needed
Medical staff from the health centres said they receive around 30 patients per month who are victims of ADF attacks. Yet the staff said their clinics receive no support from the state or from aid organisations, and that patients must self-finance their treatment.
“Most of the victims are in a state of serious vulnerability, but we too are private, unsubsidised structures,” said Pika from the Butembo clinic. “We have to buy the drugs, pay the state taxes, and pay our nursing staff. We have no choice.”
Marie-Jeanne Masika, the local NGO worker, said some displaced families have come to her organisation presenting bills of more than $300 issued by health centres for psychiatric support.
“It is too much for the victims, who have lost everything in the attacks, and these kinds of bills trouble them rather than relieve them,” said Masika, whose organisation is called Social Integration for the Promotion of the Needy (ISPRON).
Mumbere Nyerere, an ADF victim who is receiving therapy, said paying for care represents a “big difficulty”. “I am the father of the family. Those who finance my care are my parents, older than me. It is I who should assist them,” Nyerere said.
As attacks continue, Masika called for the government to subsidise clinics providing mental health support and said occupational therapy should be rolled out in villages to “tackle the problem at the base”.
Georges Machokuona, a psychosocial worker in Butembo, said livelihood support is needed too: “Once they have returned home, most of those cured are faced with challenges… linked to survival, which led some to fall ill again.”
Edited by Philip Kleinfeld.




